Not sure we are in disagreement or what the topic is. I'll guess.
There are news stories reporting on these inconclusive research papers with more zest than they deserve, and it's not just Trump. Seheult just points out something about the VA study that has been overlooked in reporting I have seen.
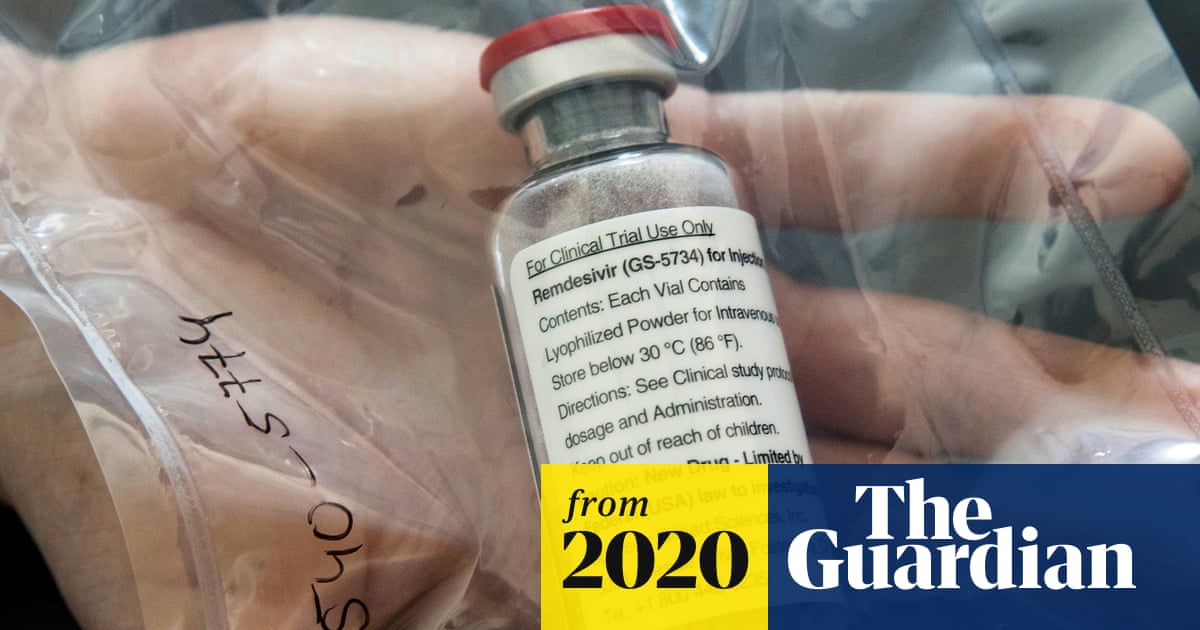
Hydroxychloroquine and remdesivir won't be the last drugs that get caught up in controversy. Seheult is educating the public on the pitfalls inherent in drug research. It is a natural extension of his work educating medical professionals.
People often have to pay for his videos. He's giving videos about COVID away for free. He has staff helping to get the videos out. He is not some guy in his mother's basement eating fruit loops!
Could you give me some more details of this chap's "work educating medical professionals," please?
He runs a website selling investment advice, with a particular emphasis, it seems to me, on encouraging people to buy precious metals, and has no professional medical qualifications that I can see --
according to his biography on his site,
Chris Martenson, PhD (Duke), MBA (Cornell) is an economic researcher and futurist specializing in energy and resource depletion
so it's unclear to me why either medical professionals or anyone else would turn to him for advice on medical matters or, indeed, any topic other than their investment portfolio.
I don't know how it works in the US, but in the UK doctors, or doctors working for the NHS certainly, follow guidance issued not by laypeople with YouTube channels but by the National Institute for Health and Care Excellence (NICE),
whose current guidance on Covid-19 is to be found here.
NICE must use the same sources for their evidence reviews as does he, and have the advantage of being medical experts rather than specialists in energy and resource depletion, and the moment, the most that can be said of all these studies about potential therapies for Covid-19 is that they suggest some particular drugs currently used to treat other conditions may be useful for Covid-19 too, but the available evidence is insufficient to allow anyone to form a firm conclusion.
That's why Oxford University and the Nuffield Foundation are running, at this moment, the large-scale clinical trials to which I referred early -- to gain sufficient evidence for sound medical decisions to be taken, and when those trials have concluded, NICE then will consider their peer-reviewed findings and update their advice as appropriate.
I'm puzzled because I don't see how this chap's YouTube channel is supposed to help in this process -- my GP's decision making is guided by NICE and her professional expertise and experience, and I'm guided by her, which is why I was puzzled by that advice that
You need to watch this video, which debunks the research which showed that hydroxychloroquine doesn't work.
The context, you will recall, is that I said my local GP is participating in clinical trials of hydroxychloroquine, which means that, should I become infected and decide to participate in the trials, I'll either be given hydroxychloroquine or a placebo,
and neither of us will, at the time, know which it is.
So I just don't understand why I "need to watch this video," or any other video about possible treatments for Covid-19.
What benefit would I gain from watching it that I wouldn't equally gain from watching any other informative video on a scientific topic (or, indeed, people's videos of their pets at play)?
I just don't see what part of my, or my doctor's, decision-making processes are supposed to be informed by this kind of video, and I'm asking someone to explain it to me -- am I supposed to show my GP the video in the hope of persuading her to prescribe me something, or what?


 www.theguardian.com
www.theguardian.com












